Urea cycle disorders (UCDs) are caused by genetic defects in the enzymes or transporter molecules of the urea cycle1
- This results in an accumulation of ammonia in the bloodstream
- Hyperammonemia can result in seizures, neurological symptoms, coma, and death
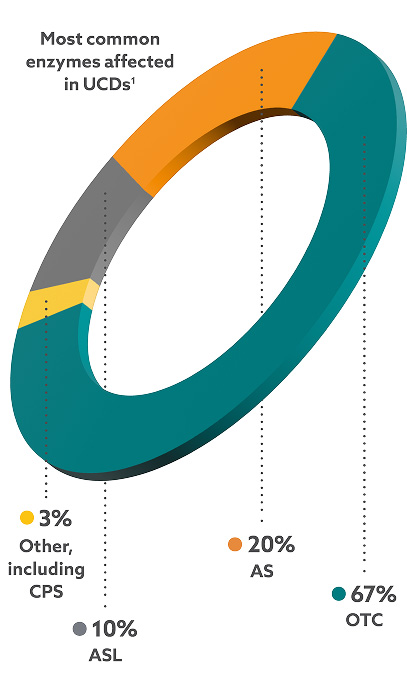
There are eight different types of UCDs, with ornithine transcarbamylase deficiency (OTCD) being the most common.1
OTCD is X-linked, therefore2:
- OTCD males tend to have severe symptoms
- OTCD females have varying degrees of symptoms, ranging from asymptomatic to severe
- About 10% of OTCD females experience noticeable symptoms
- Many have subtle symptoms that don’t trigger medical attention
- Neurological symptoms can develop even without obvious hyperammonemic events
AS, argininosuccinate acid synthetase; ASL, argininosuccinate lyase; CPS, carbamylphosphate synthetase; OTC, ornithine transcarbamylase
Uncontrolled UCDs can have serious medical consequences, including coma and death.1